

 Menu
Menu





Aneurysms – An Overview
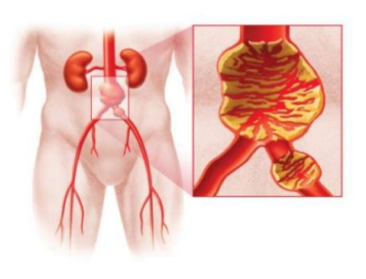
An aneurysm is an abnormal widening or ballooning of a portion of an artery due to weakness in the wall of the blood vessel.
Aneurysms are important because they can burst causing life threatening haemorrhage. This is especially true for aneurysms in the aorta.
In other locations aneurysms can also become blocked with clotted blood (thrombosed), causing a critical loss of blood supply. Thrombosis of a Popliteal aneurysm near the knee often puts the leg at risk.
Treatment depends on the size and location of the aneurysm.
Elective Surgical Repair in a timely manner before complications arise is the best approach.
Aortic Aneurysms are the most common type that need repair.
Minimally invasive repair of Aortic Aneurysms with a large Stent is the method preferred in this Practice.
Small aneurysms with little chance of complication are monitored until they grow to a size where it is safer to intervene than it is to allow nature to take its course.
The Cause of Aortic Aneurysms
Aortic aneurysms do not have a single cause.
A number of factors are implicated:
- Age – Aneurysms become more common with age. They are rare under fifty.
- Male gender – Aneurysms are more common in men. The male to female ratio for Aortic Aneurysms is about 8:1.
- Familial and Genetic Factors – Aortic Aneurysms are more common among first order relatives (children and siblings).
- Smoking – Most patients with an aneurysm smoke or have smoked. The association is quite strong.
- Hypertension
- Rare Connective Tissue Disorders – Marfan’s Syndrome is a rare disorder with weakness of the arterial wall. Marfan’s patients can develop aneurysms at an early age.
Beyond these factors the cause of aneurysms remains unknown. What causes weakness in the arterial wall has been a longstanding subject of research that has yielded few answers to date.
Treatment of Aneurysms
When to Treat Aneurysms
Aortic Aneurysms:
- Size: Treatment is considered for Abdominal Aortic Aneurysms (AAA) when the diameter reaches 50 – 55mm, and for Thoracic Aortic Aneurysms when the diameter reaches 60mm.
- Rapid Increase in Size: An increase of 10mm in a year is an indication for surgery. The average rate of growth for an AAA is 2-3mm per year. Rapid expansion in the AAA diameter is taken to indicate weakness in the wall of the Aorta.
- Symptoms: Symptoms that suggest rupture of an aneurysm is imminent are uncommon. However, they do occur from time to time, and repair of the aneurysm is then done on a semi-urgent basis. These include persistent abdominal or back pain (with no other identifiable cause), and tenderness
Principles of Treatment
Aneurysms in large arteries are treated by methods that preserve blood flow. There are two types of operation.
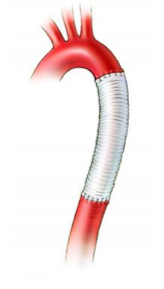
Stent Graft Repair
A stent may be placed across the aneurysm.
The stent extends from normal caliber artery above the aneurysm to normal caliber artery below. It is like an inlay tube within the artery.
The stent consists of a watertight fabric tube that contains the blood and a metal scaffold that gives it shape.

Surgical Repair
The aneurysm is replaced with a bypass that is sutured to normal caliber artery above the aneurysm and to normal caliber artery below. Diagram
For large arteries a fabric bypass is usually used. For smaller vessels a vein bypass is sometimes done.
Small aneurysms in non-essential arteries can be treated by exclusion from the circulation. There are two types of operation.
Embolization
Coils or other materials that cause the blood to clot can be placed in the aneurysm (+/- the adjacent normal artery). This prevents blood flow through the aneurysm and is an effective treatment. The coils are usually delivered through a catheter.
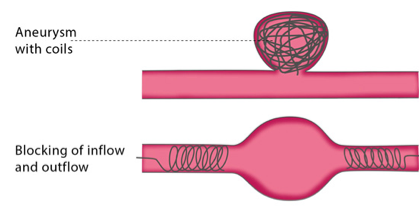
Surgical Ligation
Tying off the normal caliber artery above and below the aneurysm is also an effective way of excluding the aneurysm from the circulation. It is done when the aneurysm is easily accessible, or when embolization is not feasible.
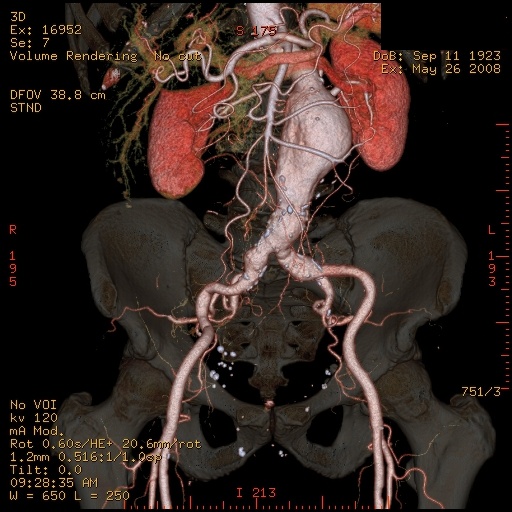
Abdominal Aortic Aneurysms (AAA)
Endovascular Aneurysm Repair (EVAR) is the term used to describe stent repair of Abdominal Aortic Aneurysms.
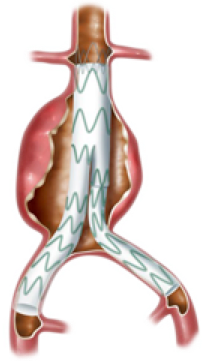
This is the modern minimally invasive method of repair.
It is the preferred method in this practice, and is used to treat 90% of our patients with AAA.
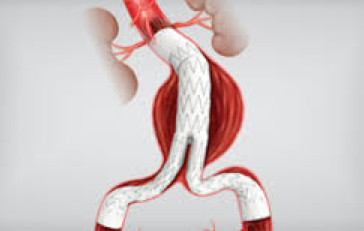
The stent is introduced through small incisions in the groin. It is assembled within the AAA.
The stent typically has 3 parts:
The main body, which attaches to normal aorta below the renal arteries, and
Two limb extensions, which pass down to the iliac arteries, (branches of the aorta in the pelvis).
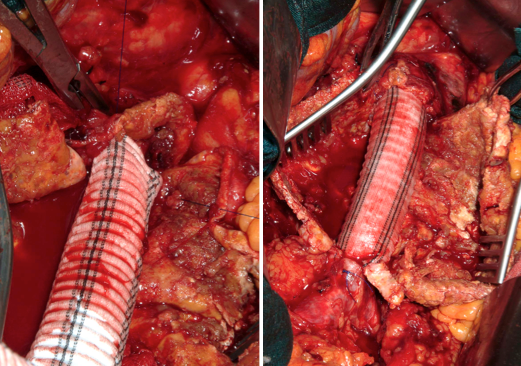
Open Surgical Repair of AAA refers to traditional operative repair.
It is more versatile than EVAR, and in this Practice is reserved for cases where EVAR cannot be done. This is about 10% of cases.
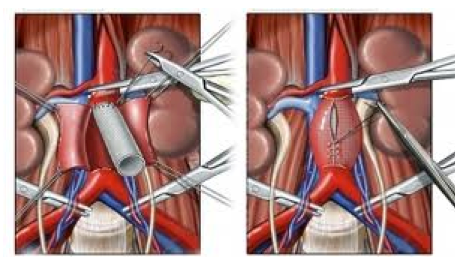
The procedure is done through a long midline abdominal incision.
A Dacron fabric tube is sutured in to replace the AAA.
Clamps are applied above and below the aneurysm while suturing takes place.
Pros and Cons
EVAR is the method of AAA repair favoured by most patients and by this Practice. Compared with open repair it has the advantages of:
- Lower operative mortality
- Fewer serious complications
- Quicker and easier recovery
- Small incisions with less discomfort
- Better tolerated by elderly patients
However, it is important to offer a dependable procedure to patients, and sometimes, due to the anatomy of the aneurysm, open repair is the only reliable method.